24/7 Careline

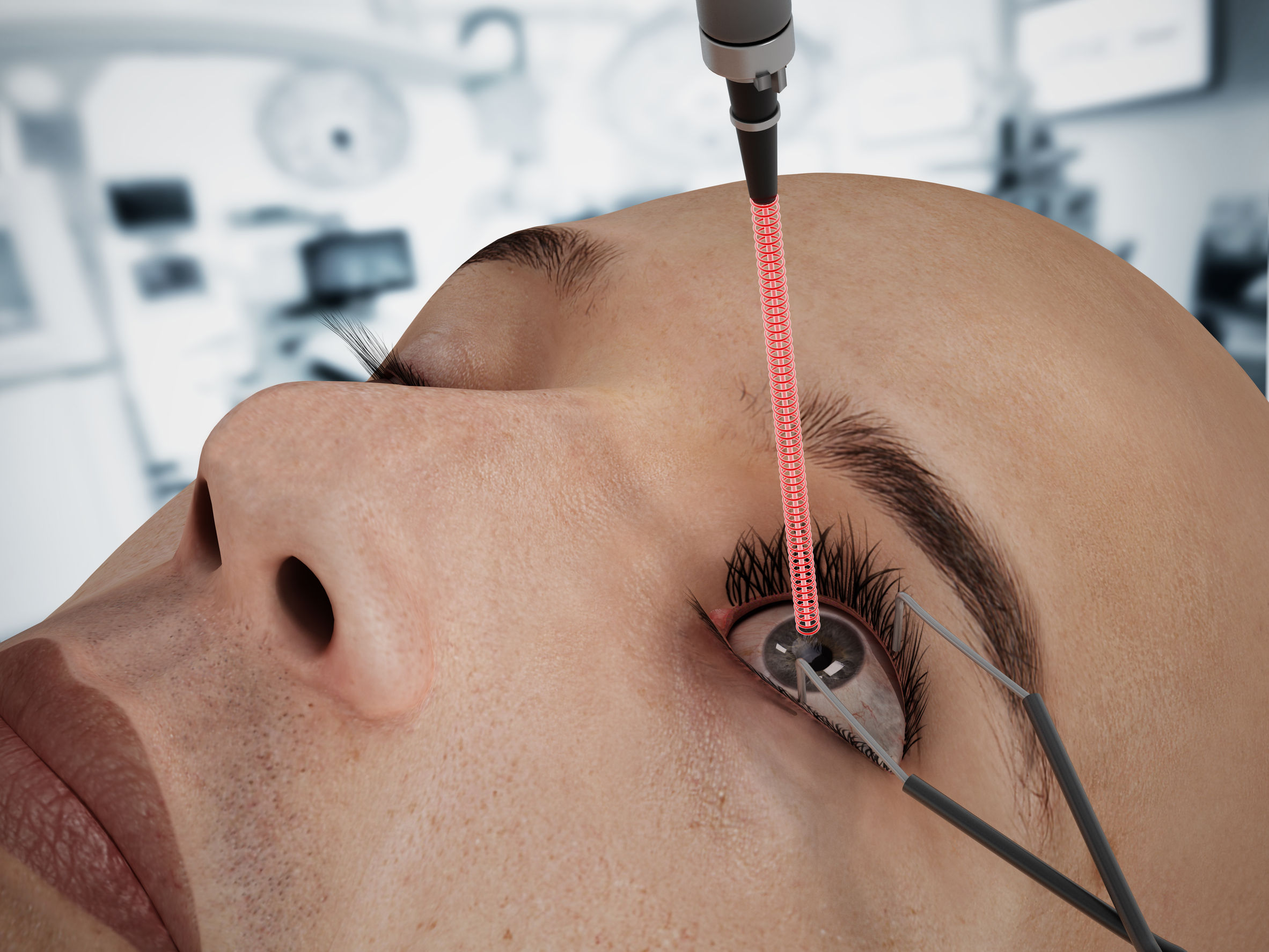
Femtosecond Laser-assisted Cataract Surgery
Cataracts, is the clouding of the natural crystalline lens within the eye, resulting in progressive blurring of vision, leading to eventual blindness if left untreated. Common symptoms of cataracts include hazy vision, difficulty reading in dim light, poor night vision, halos and glare around lights, and sometimes double vision. The definitive treatment for visually significant cataract is cataract surgery. It is estimated that, worldwide, 19 million cataract surgeries are performed annually, making it the most performed surgical procedure, with also one with the highest success rates.1
Cataract surgery is thought to be one of the oldest and earliest surgeries ever done, reportedly performed as early as the fifth century BC.2Cataract surgery has evolved, from couching, an ancient technique of cataract surgery requiring the dislocation of a dense mature cataract into the vitreous cavity via a blow to the eye, to modern surgical techniques, in which the cloudy lens is removed and clear intraocular lens (IOL) is implanted. Beginning with manual cataract extraction methods such as intra-capsular cataract extraction (ICCE), then extracapsular cataract extraction (ECCE), followed by a major advancement in 1967, when Dr. Charles Kelman introduced small incision cataract surgery via phacoemulsification (using ultrasound)3, the evolution of cataract surgery continues with the recent introduction femto-second laser-assisted cataract surgery (FLACS).

Despite the rapid advancement in technology, the principles of modern cataract surgery remains unchanged. First, an incision is created in the clear tissue called the cornea (with either a metal or diamond blade), followed by the manual creation of a circular window or opening in the capsule (a thin transparent tissue enveloping the natural lens) called capsulotomies, to allow access to the cataractous lens. The lens is divided using micro instruments introduced though the corneal incision created earlier to divide it into smaller pieces, before finally being removed from the eye through the combination of phaco-emulsification (using ultrasound energy to fracture the lens into finer pieces) and aspiration of the cataract.
In FLACS, some major steps of cataract surgery is performed automatically by the laser system. This includes the creation of access incisions in the cornea, the formation of a window or opening in the bag/capsule that envelopes the cataractous lens, mitigation of existing astigmatism of the eye through the creation of arcuate or limbal relaxing incisions, and then, the division and “softening” of the central hard portion of the cataractous lens (nucleus) in preparation for its total removal via phaco-emulsification and aspiration. Once the cataract is totally cleared from the bag, a foldable intraocular lens is then inserted and deployed.
FLACS uses a laser which fires at an ultra rapid rate, creating ultrashort pulses of a femto-second in duration. A femto-second is the SI unit of time equal to 10−15 or 1/1,000,000,000,000,000 of a second; that is, one quadrillionth, or one millionth of one billionth, of a second.4A laser fired with such short intervals allowfor the creation of tissue planes within the eye, with very little heat, and thuscollateral damage to surrounding tissues is eliminated. To date, five femto-second laser technology platforms are commercially available for cataract surgery:Catalys (Optimedica), Lensx (Alcon Laboratories, Inc.),Lensar (Lensar, Inc.), Victus (Technolas) and Femto LDV Z8 (Ziemer Ophthalmic Systems, AG).
The advent of FLACS has helped to improve cataract surgery but not without some shortfalls. Several clinical studies have indicated that femtosecond laser capsulotomies are significantly more precise in size and reproducibility than those created manually by the surgeon, resulting ina more stable refractive result with less IOL tilt anddecentration than a manual CCC, an important factor, especially with the use of toric(specialized lenses for the correction of astigmatism) and premium multi-focal intraocular lenses.5-11However, femto capsulotomies may sometimes be complicated by the production of incomplete capsular tags, which may tear, and compromise the strength of the capsulotomies in comparison to manual capsulotomies which do not have them.12Nevertheless, with improvement in software and systems, femtosecond capsulotomies are now more consistent and “free-floating”.


Fragmentation and “softening” of the cataract with the femto-laser results in shorter phaco time and hence less ultrasound energy applied to sensitive structures within the eye, particularly the endothelium of the cornea. This is beneficial in hard cataracts or in eyes with compromised corneas (with low endothelial counts). A potential complication unique to the FLACS is the formation of significant amounts of bubbles in the bag which in some instances may potentially cause a rupture in the capsule. However, even in manual division of the lens with micro-instruments, rupture of the capsule is still a potential complication. Newer femto laser systems mitigate this problem by producing less air bubbles, via lower energy systems.
The incision of the cornea by femto second laser is reported to be more stable and reproducible13, however, the jury is still out on whether these “bladeless” incisions are indeed superior to incisions created manually with a metal or diamond knife.
Visual acuity and surgical outcome with femto second laser is good, but comparison studies with conventional surgery is at the moment mixed, partly due to the lack of long term data for FLACS, but also due to the learning curve effect, and limitation of early versions of the femto laser systems. Newer versions and updates however, have continued to further improve visual result of FLACS.
In summary, femto-second laser-assisted cataract surgery offers a new armamentarium for surgeons to achieve safe and accurate surgery, allowing for consistent and reproducible surgical results which may be advantageous in certain eye conditions, and may be desired especially with the use of toric and premium multifocal lenses in which the outcome of surgery is not simply the removal of the haze caused by the cataract, but also a refractive procedure to correct refractive errors, and improve range of vision. However, it is still the responsibility of the surgeon to provide appropriate council to the patient on the potential benefits and complexities of FLACS, and if the added cost is justified, so that the patient will be able to ultimately make an informed decision on which modality is best.
By Dr Ainur Rahman; Consultant Ophthalmologist